
Anal Fistula –...
Introduction Anal fistula is a medical condition that often goes unnoticed or misunderstood. In this comprehensive guide, we'll delve into the causes,...
Read More
On #Doctor’sDay, allow...
It is sad and surprising we never think or talk about the most inevitable moment of our lives. Discussing it is said...
Read More
“Science is not...
The men practising the science of medicine are an esoteric lot who commanded a lot of respect. Till recently. And then the...
Read More
Back To The...
If you look at the bigger picture, food, clothes and a house can be viewed as tools to survive. Purely functional at...
Read More
Human Bias Is...
Human bias is like a virus. We have it and we don’t know we have it. A large majority of us have...
Read More
Bariatric Surgery- Your...
We keep telling our patients that bariatric surgery is not a magic pill. Neither is it a quick-fix to lose all your...
Read More
Do Not Take...
Heartburns have become so commonplace in modern life that many have started believing it’s the new normal. However, it’s definitely a disease...
Read More
Bariatric surgery for...
Is your child obese? Does he sit quietly in the house not wanting to go to school or play with other children?...
Read More
Fatty liver? Cirrhosis?...
Liver disease is not uncommon in India. A few years back, the commonest cause was viral hepatitis. Recently, obesity has become the...
Read More
Are We Letting...
Modern life, whatever it means, has made us strive for more. All of us have this innate desire to progress and grow...
Read More
Hernia Workshop At...
Recently I had an opportunity to visit the Philippines as an invited faculty for a Hernia workshop The opportunity resulted when one...
Read More
Types Of Bariatric...
India ranks third in terms of having obese individuals only after US and China. One in every five Indian is either overweight...
Read More
How To Choose...
In a unique event on Sunday 23rd July at the Hotel Taj Bengal, organized by Dr. Sarfaraz J Baig, who played the...
Read More
How To Choose...
The medicine and medical professionals have always been treated with utmost respect in every corner of the world, irrespective of the race,...
Read More
The failing doctor-patient...
Now that the doctors nationwide are crying foul over the allegations against them by the media and the politicians, time has come...
Read More
What Do Real...
I travel the World a lot for seeing the masters of their discipline. And there are many things in common to all...
Read More
A Brief Guide...
Gastric Reflux (GERD) refers to the regurgitation of acid stomach contents into the esophagus. The most common clinical manifestation of GERD is heartburn...
Read MoreThe Basic Concept...
Very late in the day I realized that Nutrition was my calling. As all women I suffered midlife crisis with ample time...
Read More
Intermittent Fasting for...
Fasting has been an integral part on all religion. Our forefathers have practiced fasting on a regular basis. Monks eat food sparingly,...
Read More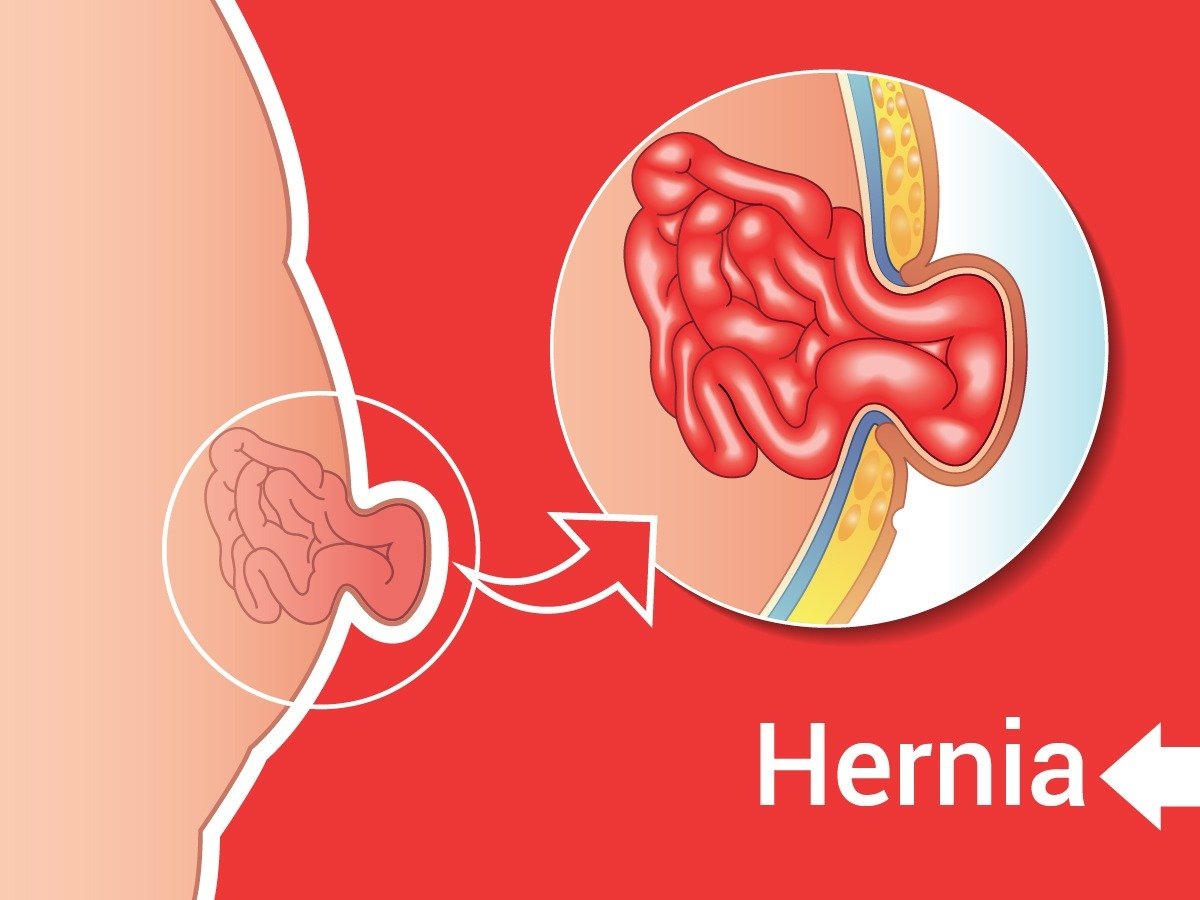
TAR Comes as...
New surgery (TAR) for failed hernia repair gives new life to frustrated patients. Hernia surgery has undergone a sea of change. The...
Read More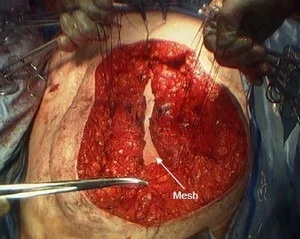
Transversus Abdominis Release...
I am sure once in a while you stumble into a large defect hernia that fails to all the conventional repair. It's...
Read More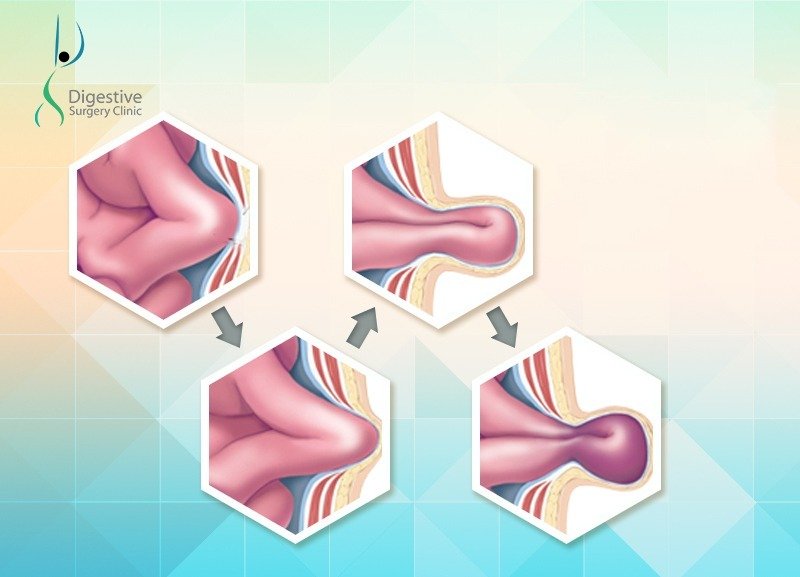
Laparoscopic Ventral Hernia...
Hernia surgery is undergoing continuous change in technique to improve results and to meet high expectations of the patient. No more is...
Read More
Chronic Pancreatitis –...
Here is a case of chronic pancreatitis that was managed surgically at our center. A 40 year old diabetic female was referred...
Read More
Abdominal Sepsis Treatment...
A 35 year old woman was referred to Digestive Surgery Clinic with abdominal sepsis following a cholecystectomy on her 11th postoperative day....
Read More
A Show of...
Obesity is one of the biggest diseases of our times. The damage it incurs on individual health, quality of life and on...
Read More
Laparoscopic Surgery is...
Colon cancer are among'st those cancers that fare better than the other abdominal cancers. The mainstay therapy is surgical removal of the...
Read More
Arthritis, Obesity and...
Obese people frequently have knee pain that makes walking painful. This is more common with advancing age. It prevents them from walking,...
Read More
Heartburns? A Laparoscopic...
1. Heartburns can be a source of great discomfort. Typically, it is brought on by eating spicy food. Many patients also have...
Read More
Snoring, Obesity and...
Most people would like to dismiss their snoring as a normal phenomenon during sleep. They feel it's the spouses who are the...
Read More
The Secret of...
Hernias are defects in the abdominal wall because of which organs from within the abdomen tend to come out just below the...
Read More
Fight Hunger! Stay...
The festive season has started since Eid and the Pujas and it is likely that the spirit will continue till the Christmas...
Read More
Skipping Breakfast –...
Conventional wisdom has always recommended a large and healthy breakfast claiming BIG health benefits. However, this has been challenged in recent times....
Read More
Eat Fat to...
Eating fat makes us fat. Right? Wrong! Continue reading Eat Fat to Lose Fat!
Read More
Anal Symptoms that...
Worried about certain prevailing conditions in your body? Here are some questions and their answers which will help you to understand the...
Read More
Fasting is only...
Fasting is only a religious ritual! Right? Wrong! In this month of fasting that many of us observe only for religious reasons,...
Read MoreActions speak louder...
In an article published in The Times of India, Dr. Sarfaraz Baig has expressed his views on advertisements which claims ‘100% guaranteed’...
Read More
Stomach cancer- what’s...
Stomach cancer is a dreaded disease. If not detected early, it progresses fast and has a poor outcome. However, in recent times,...
Read More
How many times...
Very few, most would guess. In a recently organised training program on bariatric surgery in Belle Vue, eight surgeons from West Bengal...
Read More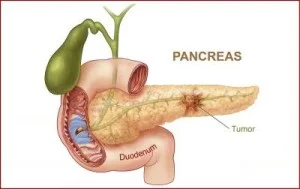
An insight into...
Diseases of the pancreas have been enigmatic from the time we have known them. Scientific progress in the field has made the...
Read More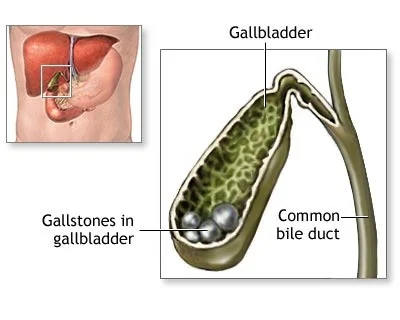
Stones in the...
It is very interesting that a human body may produce stones within it. A human body is otherwise all about flesh, fluid...
Read More
A Surgery can...
Everyone is scared of surgery! And why should one not be? The entire process involves tedious hospital admission, injections, operation and postoperative...
Read More
I have Hernia....
It's disheartening for any patient to know that their abdominal wall gave way spontaneously or after a surgery. A second surgery with...
Read More
In 2015, lets...
Health should be one of the top priorities in an individual’s life. Unfortunately it only figures frequently in a New Year’s resolution...
Read More
Surgery for Liver...
Have you known anyone who has been diagnosed with a liver tumor or cyst that needs surgery? If you do, you would...
Read MoreAnorectal diseases such...
Anus and rectum can be afflicted by diseases such as piles, fistula, fissure, rectal prolapse and cancers. The first four are common...
Read More
Mini Gastric Bypass...
The Occam’s Razor suggests that entities should not be multiplied endlessly. Although it is true in many situations, in some fields where...
Read More
Laparoscopic surgery has...
Laparoscopic surgery has revolutionised the way we do abdominal surgery. In more than two decades now it is now used for almost...
Read MoreI would rather...
If I were a diabetic, often I ask myself- would I take a surgery that promises to halt the disease, even for...
Read MoreCommon Queries and...
I write this article for my readers who may also have visited me for the consultation for bariatric surgery but have opted...
Read MoreModern Treatment of...
I have anal fistula. I have taken various medicines prescribed by alternative medical practitioners but it has not healed. I am scared...
Read MoreA Newer Bariatric...
Bariatric surgery – a weight loss surgery- is becoming an increasingly popular option for patients who are obese and diabetic. It not...
Read MoreSurgery for Hiatus...
What is a Hiatus hernia ? In a hiatus hernia, a part of the stomach that should normally be in the abdomen...
Read MoreObesity in Women...
A woman needs to preserve her beauty and health even more when she turns forty. This is because her body – and...
Read MoreResearch proves yet...
In a recent research called the STAMPEDE trial- from Cleveland Clinic, USA,a comparison was done between diabetic patients managed on medicines versus...
Read MoreHOW TO DECIDE...
Last year two boys Ramesh and Piyush (names changed) aged 19 and 22 attended our obesity clinic in Belle Vue. They were...
Read MoreCOLORECTAL AND ANAL...
Colorectal surgery (surgery of food pipes) is done for various diseases such as cancers, inflammatory bowel disease, diverticulitis and rectal prolapse. The...
Read MoreGall bladder Stones...
Why do gallstones form? Gallstones are so common in West Bengal that we can safely presume that everybody knows at least one...
Read MoreWhy is the...
Obesity has become the most important epidemic of our times. It is responsible for many diseases such as diabetes, hypertension, heart disease,...
Read MoreJaundice may be...
There are many reasons of having jaundice. On many occasions, jaundice is due to medical diseases like hepatitis requiring medicines only. Sometimes...
Read MoreMini Gastric Bypass...
The Occam’s Razor suggests that entities should not be multiplied endlessly. Although it is true in many situations, in some fields where...
Read MoreA New Approach...
What is the conventional treatment of Diabetes? Diabetes is conventionally treated by a low sugar diet, physical activity and medicines that lower...
Read MoreTREATMENT OF CHRONIC...
What is Chronic Pancreatitis? Chronic pancreatitis is a diseaseof the pancreas in which the pancreas gets progressively destroyed. It is seen in...
Read MoreDo you have...
What is Heartburn? Heartburn is the feeling of burning sensation in the upper abdomen or the central chest. This happens when the...
Read MoreCancers in the...
Nobody wants to listen to bad news. That is why, we do not want to accept any deadly diagnosis such as cancer...
Read MoreThree times failed...
Mrs Swati (name changed), 45 years old woman had already been operated three times for her hernia. Despite that, she was suffering...
Read MoreBleeding, pain and...
No. Although most of the symptoms of bleed and pain during defecation are due to piles and fissure, sometimes it may be...
Read MoreBariatric Surgery can...
Infertility in females is a growing problem. Statistics show that one in six couples are infertile. Forty percent of the problem lies...
Read MoreWhat is new...
Can gallstones be managed on medicines (without surgery)? In certain situations, some patients with asymptomatic gallstones can be managed by “wait...
Read MoreBariatric Surgery is...
I always love to answer this question. Most severely-obese patients are ready to undergo bariatric surgery (stomach stapling surgery for the severely...
Read MoreBlood in stool,...
It is interesting to ask ourselves that if the great Napolean did not have piles , would he have won more battles....
Read MoreDiseases of the...
Pancreas is an important organ in the human body responsible for digestive process and production of insulin that maintains normal glucose levels...
Read MoreNew approaches in...
There will be many procedures to choose from. However it is believed that these complex hernias should be repaired with a mesh-...
Read MoreVAAFT- Modern Treatment...
What is Anal Fistula? An anal fistula is an abnormal tract between skin and the anus. Stool enters this tract and causes...
Read MoreWhen to consider...
Good question? Obviously, one is not asking all diabetics to be subjected to surgery. Instead it is proposed as an option for...
Read More
The Demerits of...
Alcohol has been in the center of a lot of research in the past few decades for a lot of reasons. While...
Read MoreCancers in the...
Nobody wants to listen to bad news. That is why, we do not want to accept any deadly diagnosis such as cancer...
Read More
Cancers in the...
Nobody wants to listen to bad news. That is why, we do not want to accept any deadly diagnosis such as cancer....
Read More
Bariatric Surgery Can...
Infertility in females is a growing problem. Statistics show that one in six couples are infertile. Forty percent of the problem lies...
Read More
Scarless Surgery For...
Scars on the body make an ugly sight. Some do not mind, some may accept it but some just refuse to stomach...
Read More
What You Need...
'Hernias are bulges in the belly where intestines and abdominal fat come out under the skin through an abnormal opening. The abnormal...
Read More